Mattress Guides
Best Mattresses of 2024
Nowadays, there seems to be an overabundance of choice when it comes to mattresses. Far...
At Healthy Americans, we pride ourselves on the quality, research, and transparency we put into every article.

Articles are thoroughly researched

Reviewed by medical experts

Fact-checked and science-based

Frequently updated with latest findings
Nowadays, there seems to be an overabundance of choice when it comes to mattresses. Far...
According to the American Chiropractic Association, roughly 80% of individuals will suffer from back pain...
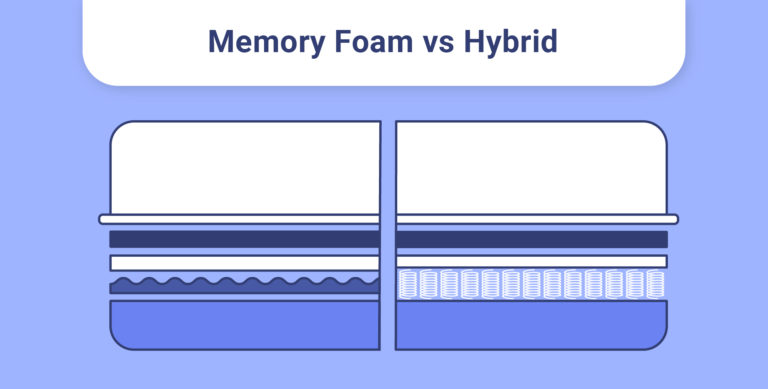
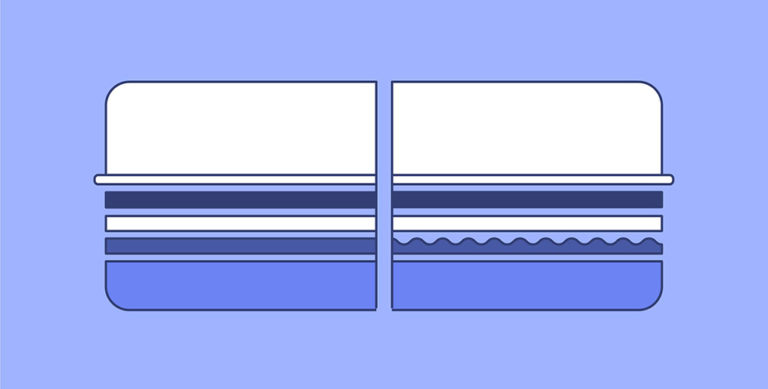
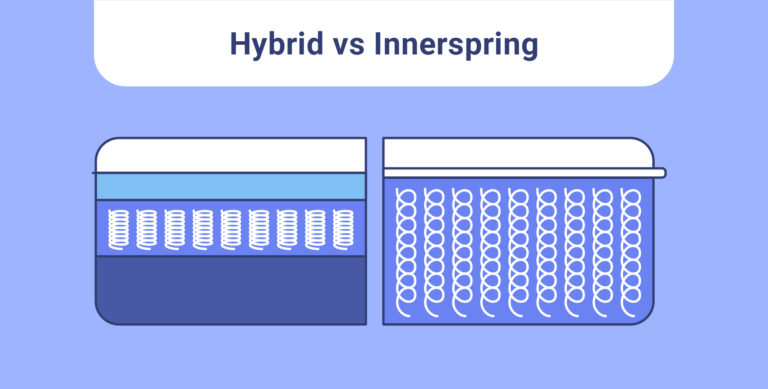
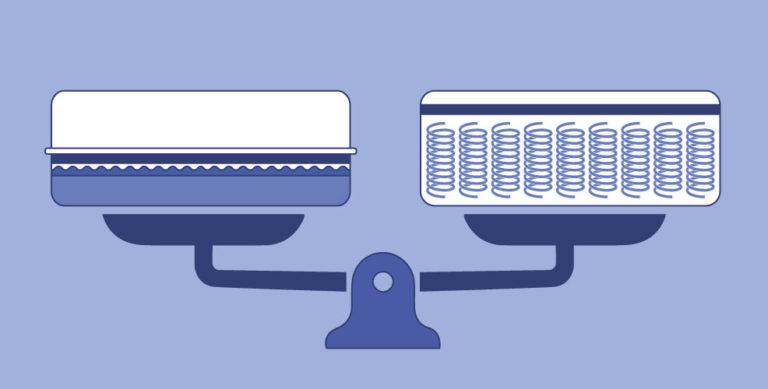
Hybrid mattresses are one of the best sleep technology developments since the invention of the...

It’s never been a better time to be a side sleeper! Side sleepers have tons...
Making sure your mattress stays clean throughout the year is essential to keeping your bed...
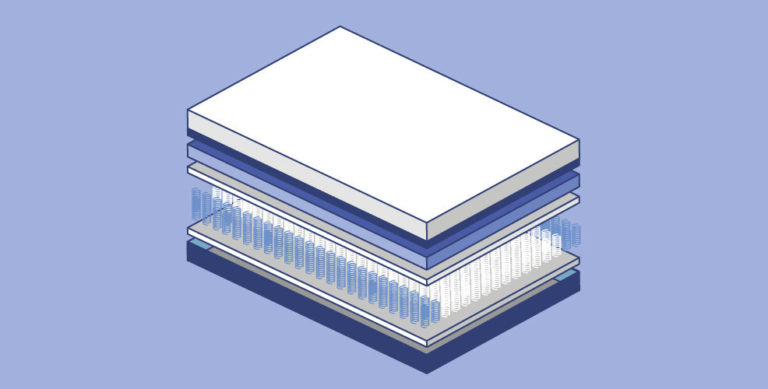
Hybrid beds are becoming popular for their soft comfort and bouncy support. Unlike traditional beds,...
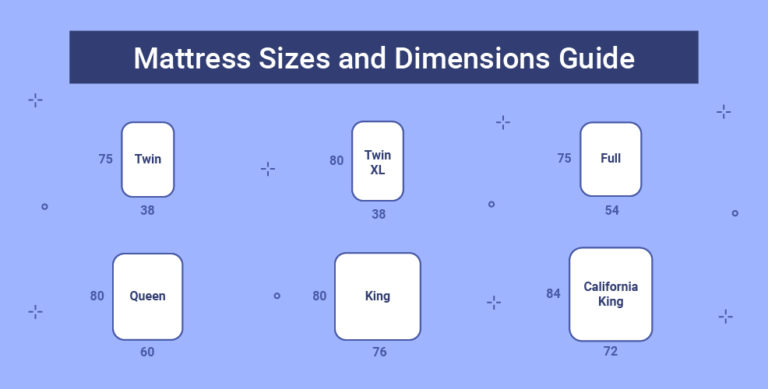
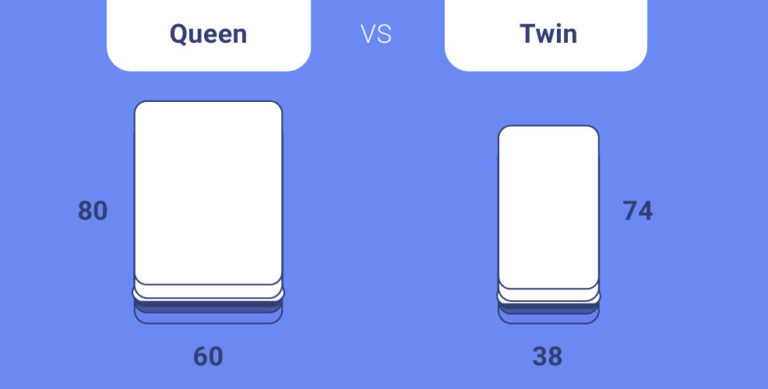
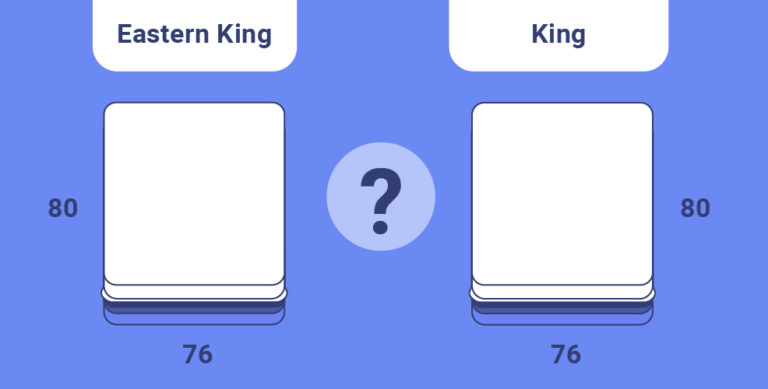
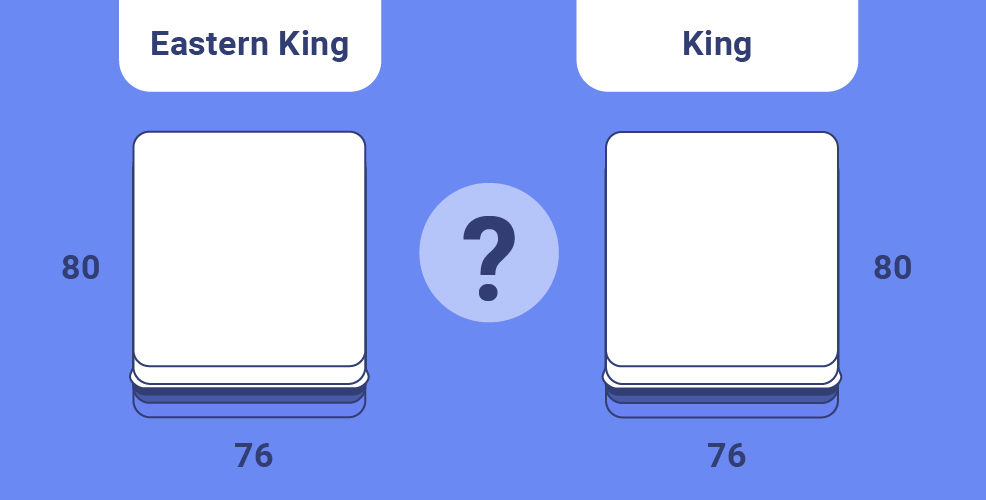
What size of mattress you choose for yourself and your children matters. Mattress size impacts...
Just like everything else, mattresses eventually wear out: They get saggy. Their springs lose tension....
The EachNight writing team is devoted to creating articles that are not only entertaining and easy to understand but also as impartial, accurate, and well-sourced as possible. Whenever possible, we strive to have our articles fact-checked by our independent review board. We also do not tolerate plagiarism or ill intent from our contributors.
Here are the medical and factual guidelines that a EachNight article must adhere to:
Our writers are sleep coaches certified by the Spencer Institute, which has been training coaches since 1992. Becoming a certified sleep coach means that our writers are well-versed in various sleep science matters, taking us beyond being just a group of mattress reviewers. The certification allows us an in-depth understanding of what we’re talking about when it comes to advising readers on better sleep habits.